Self and Others: Object Relations Theory in Practice, N. Gregory Hamilton (1988)
Basic Definitions
Object relations are interactions between the self and objects, external and internal objects. An external object is an actual person. An internal object is a mental representation of a person. The self consists of the conscious and unconscious mental representations the self. An object relations unit is a self-representation and an object-representation connected by an affect.
Mahler’s Stages of Separation-Individuation
Margaret Mahler wrote that there are four stages in what she called the psychological birth of the human infant. These stages can also be seen as the stages the infant takes as she separates and individuates from her mother.
Stage #1: Autism (0-2 months). We’re born into an undifferentiated state, unable to differentiate the self from the environment.
Stage #2: Symbiosis (2-6 months). We then enter into a state of symbiosis, having a vague awareness of mother but believing that we are both part of the same “omnipotent system,” “a dual unity with one common boundary.”
Stage #3: Separation-Individuation (6-24 months). This phase has three subphases.
Psychological Mechanisms
Our most problematic psychoanalytic patients display psychological mechanisms that correspond to what Mahler observed in young children. We thus have two lines of evidence for the psychological mechanisms of young children — our observations of young children and our observations of our patients.
Integration is the ability to bring together two mental events — for example, recognizing that the soothing mother and the angry mother are the same mother. Differentiation is the ability to set apart two mental events — for example, the ability to see that the mother is different than the father.
In projection we attribute unwanted aspects of the self — be it the mother-self unit or the individuated self — to things outside the self.
Incorporation involves taking in an external object and making it part of the self; the two become an undifferentiated one. Introjection involves taking in an external object or an aspect of an external object; the two do not become one but remain differentiated. An example of introjection is a patient who during times of distress can hear her therapist’s words of comfort; the patient knows that she is not hallucinating and that the words are coming from her own mind. Identification involves taking in qualities of a previously introjected object and making them part of one’s self-image. An example of identification would be the above patient who in time no longer hears her therapist speak words of comfort when distressed but now speaks words of comfort to herself, these words not bringing to mind the therapist although they were initially informed by the therapist.
Splitting involves keeping apart contradictory aspects of the self and objects. Idealization involves seeing the self or an object as perfect. Devaluation involves seeing the self or an object as worthless. Projective identification involves projecting an aspect of the self onto an object and then attempting to control that projected aspect of the self in the object. An example of projective identification is a patient who wants to neglect her family; she projects this feeling onto her therapist and family, believing that they are neglecting her; she responds to this perceived neglectfulness by saying that she in turn is going to neglect them.
A transitional object is “neither self nor object” but “has the qualities of both.” A teddy bear, for instance, “may be treated as if it is the beloved mother and simultaneously as if it is the beloved self.”
Maturity involves integration of different aspects of the self and integration of one’s objects. Identity consolidation involves bringing together all-good and all-bad self-images and thus seeing ourselves as being essentially good while also possessing some undesirable qualities. Object constancy involves seeing our objects as essentially good while also possessing some undesirable qualities; this is Klein’s depressive position.
Descriptive Developmental Diagnosis
Many clinicians have noticed a correspondence between patient functioning and the functioning of children at specific developmental stages.
The schizophrenic struggles with differentiation, as she has difficulty differentiating between the self and objects (external and/or internal objects). During a hallucination, for instance, she experiences something as an object that should be experienced as part of the self.
When manic, the bipolar individual displays the omnipotent mentality of the toddler in the practicing stage. When depressed, the bipolar individual displays the insecurity and smallness reminiscent of a toddler wishing to return to mother’s total care.
The individual with borderline personality disorder lacks object constancy and relies on the defense mechanisms of splitting, idealization, devaluation, and projective identification. A gratifying object is seen as all-good and becomes all-bad once it becomes frustrating. She lacks identity consolidation, seeing herself as either all-good or all-bad.
The narcissist depends on others for self-esteem maintenance. When others fail to provide adulation, the narcissist maintains her self-esteem by projecting her feelings of defectiveness onto the object. The narcissist aso struggles with integration. She has difficulty integrating grandiose and devalued aspects of self. And she can merge with idealized others, but she quickly devalues and discards them once they disappoint him.
The neurotic possesses object constancy and identity consolidation. The neurotic’s symptoms tend to be guilt, depression, and sadness, the reason being that she realizes that the object she wants to punish is the same object whom she loves. The neurotic relies on repression, not splitting. In repression, one experiences conflicted feelings at the same time and tries to remain unaware of one of the conflicted feelings; this is different than splitting, where one feeling is experienced consciously at one time and the opposite feeling at another time with little sense of conflict, either conscious or unconscious.
Therapeutic Action
Therapeutic action describes how it is that therapy brings about change. Object relations holds that therapy brings about change through the therapist’s technical interventions as well as by the real relationship that exists between the therapist and patient.
Technical Interventions
Clarification, Confrontation, and Interpretation. The primary technical interventions used by the object relations analyst are essentially the same as those used by classical analysts: clarification, confrontation, and interpretation. Clarification involves asking for more information. Confrontation involves verbally making an observation about the patient.
Interpretation involves pointing out a parallel between a past event and the patient’s current life or a past event and something happening in the transference. When we make an interpretation for a patient who uses repression, we are “facilitating the memory of a previously existing association”. When we make an interpretation for a patient who uses splitting, we are creating an association between two events, e.g., showing that a present feeling is a repetition of a former feeling.
Confronting Frame Violations. We need to regularly confront frame violations with borderline patients in order to clarify self-others boundaries and in so doing to facilitate the development of object constancy.
Setting Limits. When confrontation is not enough, we need to set limits, which means we need to explain the consequence for continued frame violations. The only consequences we can make are ending therapy or breaking confidentiality.
Confronting Negative Transference. It might be necessary to confront negative transference early on with a borderline patient . A negative transference is the projection of a bad internal object onto the therapist. Here’s an example of such a confrontation. Patient: “I feel horrible and alone. No one understands me anyway. What’s the use? I don’t even know why I come here.” Therapist: “You must be disappointed in me. You hired me to try to understand you and help you, but you still feel like no one understands you.” Patient: “No, no. It’s not you. You are the only one who cares. I feel so much better when I’m here. It’s that bastard husband of mine — and my mother.”
Real Relationship
The therapeutic relationship involves both fantasy and reality. The fantasy is found in the patient’s transference, as the patient projects her own object-images onto the therapist. The reality is found in the real relationship, as the patient sees the therapist, not only as a projection of object-images, but also as a real person. The reality of the relationship is referred to as the real relationship, and this relationship brings about change in a number of ways.
Container. Bion developed the idea of the container. He observed that “infants often become overwhelmed by extreme and unmodulated affects and communicate these feelings in their facial expressions, cries, and coos. By listening and watching, the attentive parent takes in these communicated feelings, modulates them, transforms them, gives them meaning, and returns them to the child. The child eventually internalizes this process and learns to contain his own affects.” In a similar way, the therapeutic “framework of quiet listening, uninterrupted hours, and modulated and interested responses provides a containing function.”
Holding Environment. The idea of the container is similar to Winnicott’s idea of the holding environment. The good enough mother holds the child — at first she holds the child physically, and as the child matures, she holds the child in her attention. Similarly, the good enough therapist holds patient’s in her attention.
Empathy. Empathy “contributes to the containing and holding aspects of the therapeutic relationship.” Empathy can work as projective identification to help us to understand the patient, as we project our self-image onto the patient to understand how she feels.
Titrating Closeness. The attuned therapist continuously keeps the right distance between herself and the patient. She can move closer to the patient by doing such things as leaning closer in her chair and by making empathic statements. If the patient shows signs of anxiety, this might indicate the patient’s fear of fusing with the patient and thus losing her loss of self, and the therapist responds by moving further away.
Positive Projective Identification. An example of this would be a therapist working with a man who has been denigrated by others in his life. The therapist believes the man is valuable and treats him as such. In so doing, the therapist has projected her own self-images and object-images of a valuable human being onto the patient and treated him accordingly.
Object relations are interactions between the self and objects, external and internal objects. An external object is an actual person. An internal object is a mental representation of a person. The self consists of the conscious and unconscious mental representations the self. An object relations unit is a self-representation and an object-representation connected by an affect.
Mahler’s Stages of Separation-Individuation
Margaret Mahler wrote that there are four stages in what she called the psychological birth of the human infant. These stages can also be seen as the stages the infant takes as she separates and individuates from her mother.
Stage #1: Autism (0-2 months). We’re born into an undifferentiated state, unable to differentiate the self from the environment.
Stage #2: Symbiosis (2-6 months). We then enter into a state of symbiosis, having a vague awareness of mother but believing that we are both part of the same “omnipotent system,” “a dual unity with one common boundary.”
Stage #3: Separation-Individuation (6-24 months). This phase has three subphases.
Subphase #1: Hatching (6-10 months). We begin to individuate, studying the mother’s face, taking an interest in other people.
Subphase #2: Practicing (10-16 months). We begin to practice ego functions and experience joy as we do so; we begin to toddle around and explore the environment, using the mother for refueling.
Subphase #3: Rapprochement (16-24 months). We realize that our new independence brings about separation from the mother, and we respond with anxiety and become clingy.
Stage #4: Object Constancy (24-36 months). When we have obtained individuality, we have a stable sense of self that persists through different situations and moods. When we have obtained object constancy, we can hold a steady image of objects, especially the mother, even when the object is absent, even when the object is not gratifying.
Stage #4: Object Constancy (24-36 months). When we have obtained individuality, we have a stable sense of self that persists through different situations and moods. When we have obtained object constancy, we can hold a steady image of objects, especially the mother, even when the object is absent, even when the object is not gratifying.
Psychological Mechanisms
Our most problematic psychoanalytic patients display psychological mechanisms that correspond to what Mahler observed in young children. We thus have two lines of evidence for the psychological mechanisms of young children — our observations of young children and our observations of our patients.
Integration is the ability to bring together two mental events — for example, recognizing that the soothing mother and the angry mother are the same mother. Differentiation is the ability to set apart two mental events — for example, the ability to see that the mother is different than the father.
In projection we attribute unwanted aspects of the self — be it the mother-self unit or the individuated self — to things outside the self.
Incorporation involves taking in an external object and making it part of the self; the two become an undifferentiated one. Introjection involves taking in an external object or an aspect of an external object; the two do not become one but remain differentiated. An example of introjection is a patient who during times of distress can hear her therapist’s words of comfort; the patient knows that she is not hallucinating and that the words are coming from her own mind. Identification involves taking in qualities of a previously introjected object and making them part of one’s self-image. An example of identification would be the above patient who in time no longer hears her therapist speak words of comfort when distressed but now speaks words of comfort to herself, these words not bringing to mind the therapist although they were initially informed by the therapist.
Splitting involves keeping apart contradictory aspects of the self and objects. Idealization involves seeing the self or an object as perfect. Devaluation involves seeing the self or an object as worthless. Projective identification involves projecting an aspect of the self onto an object and then attempting to control that projected aspect of the self in the object. An example of projective identification is a patient who wants to neglect her family; she projects this feeling onto her therapist and family, believing that they are neglecting her; she responds to this perceived neglectfulness by saying that she in turn is going to neglect them.
A transitional object is “neither self nor object” but “has the qualities of both.” A teddy bear, for instance, “may be treated as if it is the beloved mother and simultaneously as if it is the beloved self.”
Maturity involves integration of different aspects of the self and integration of one’s objects. Identity consolidation involves bringing together all-good and all-bad self-images and thus seeing ourselves as being essentially good while also possessing some undesirable qualities. Object constancy involves seeing our objects as essentially good while also possessing some undesirable qualities; this is Klein’s depressive position.
Descriptive Developmental Diagnosis
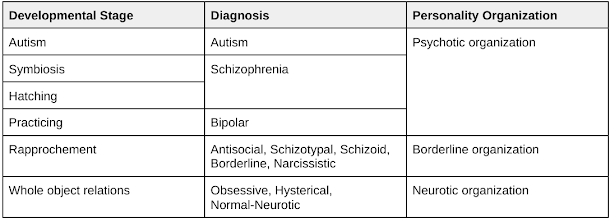
Many clinicians have noticed a correspondence between patient functioning and the functioning of children at specific developmental stages.
The schizophrenic struggles with differentiation, as she has difficulty differentiating between the self and objects (external and/or internal objects). During a hallucination, for instance, she experiences something as an object that should be experienced as part of the self.
When manic, the bipolar individual displays the omnipotent mentality of the toddler in the practicing stage. When depressed, the bipolar individual displays the insecurity and smallness reminiscent of a toddler wishing to return to mother’s total care.
The individual with borderline personality disorder lacks object constancy and relies on the defense mechanisms of splitting, idealization, devaluation, and projective identification. A gratifying object is seen as all-good and becomes all-bad once it becomes frustrating. She lacks identity consolidation, seeing herself as either all-good or all-bad.
The narcissist depends on others for self-esteem maintenance. When others fail to provide adulation, the narcissist maintains her self-esteem by projecting her feelings of defectiveness onto the object. The narcissist aso struggles with integration. She has difficulty integrating grandiose and devalued aspects of self. And she can merge with idealized others, but she quickly devalues and discards them once they disappoint him.
The neurotic possesses object constancy and identity consolidation. The neurotic’s symptoms tend to be guilt, depression, and sadness, the reason being that she realizes that the object she wants to punish is the same object whom she loves. The neurotic relies on repression, not splitting. In repression, one experiences conflicted feelings at the same time and tries to remain unaware of one of the conflicted feelings; this is different than splitting, where one feeling is experienced consciously at one time and the opposite feeling at another time with little sense of conflict, either conscious or unconscious.
Therapeutic Action
Therapeutic action describes how it is that therapy brings about change. Object relations holds that therapy brings about change through the therapist’s technical interventions as well as by the real relationship that exists between the therapist and patient.
Technical Interventions
Clarification, Confrontation, and Interpretation. The primary technical interventions used by the object relations analyst are essentially the same as those used by classical analysts: clarification, confrontation, and interpretation. Clarification involves asking for more information. Confrontation involves verbally making an observation about the patient.
Interpretation involves pointing out a parallel between a past event and the patient’s current life or a past event and something happening in the transference. When we make an interpretation for a patient who uses repression, we are “facilitating the memory of a previously existing association”. When we make an interpretation for a patient who uses splitting, we are creating an association between two events, e.g., showing that a present feeling is a repetition of a former feeling.
Confronting Frame Violations. We need to regularly confront frame violations with borderline patients in order to clarify self-others boundaries and in so doing to facilitate the development of object constancy.
Setting Limits. When confrontation is not enough, we need to set limits, which means we need to explain the consequence for continued frame violations. The only consequences we can make are ending therapy or breaking confidentiality.
Confronting Negative Transference. It might be necessary to confront negative transference early on with a borderline patient . A negative transference is the projection of a bad internal object onto the therapist. Here’s an example of such a confrontation. Patient: “I feel horrible and alone. No one understands me anyway. What’s the use? I don’t even know why I come here.” Therapist: “You must be disappointed in me. You hired me to try to understand you and help you, but you still feel like no one understands you.” Patient: “No, no. It’s not you. You are the only one who cares. I feel so much better when I’m here. It’s that bastard husband of mine — and my mother.”
Real Relationship
The therapeutic relationship involves both fantasy and reality. The fantasy is found in the patient’s transference, as the patient projects her own object-images onto the therapist. The reality is found in the real relationship, as the patient sees the therapist, not only as a projection of object-images, but also as a real person. The reality of the relationship is referred to as the real relationship, and this relationship brings about change in a number of ways.
Container. Bion developed the idea of the container. He observed that “infants often become overwhelmed by extreme and unmodulated affects and communicate these feelings in their facial expressions, cries, and coos. By listening and watching, the attentive parent takes in these communicated feelings, modulates them, transforms them, gives them meaning, and returns them to the child. The child eventually internalizes this process and learns to contain his own affects.” In a similar way, the therapeutic “framework of quiet listening, uninterrupted hours, and modulated and interested responses provides a containing function.”
Holding Environment. The idea of the container is similar to Winnicott’s idea of the holding environment. The good enough mother holds the child — at first she holds the child physically, and as the child matures, she holds the child in her attention. Similarly, the good enough therapist holds patient’s in her attention.
Empathy. Empathy “contributes to the containing and holding aspects of the therapeutic relationship.” Empathy can work as projective identification to help us to understand the patient, as we project our self-image onto the patient to understand how she feels.
Titrating Closeness. The attuned therapist continuously keeps the right distance between herself and the patient. She can move closer to the patient by doing such things as leaning closer in her chair and by making empathic statements. If the patient shows signs of anxiety, this might indicate the patient’s fear of fusing with the patient and thus losing her loss of self, and the therapist responds by moving further away.
Positive Projective Identification. An example of this would be a therapist working with a man who has been denigrated by others in his life. The therapist believes the man is valuable and treats him as such. In so doing, the therapist has projected her own self-images and object-images of a valuable human being onto the patient and treated him accordingly.
Comments
Post a Comment